
IBS and SIBO - What a pelvic health provider needs to know
If you treat people with pelvic pain or pelvic floor dysfunction, this is why you should care
IBS is an intestinal disorder characterized by chronic or recurrent lower abdominal pain or discomfort associated with altered stool consistency and frequency. It’s also the most common gastrointestinal dysfunction associated with chronic pelvic pain (CPP), affecting 50% of such women presenting to gynecologic clinics.

But wait, there’s more….
Although there are different types of IBS, the prevalence of SIBO is significantly increased in those with IBS compared to controls. Additionally, one small study found that 81% of patients with IC/PBS had a positive breath test for SIBO.
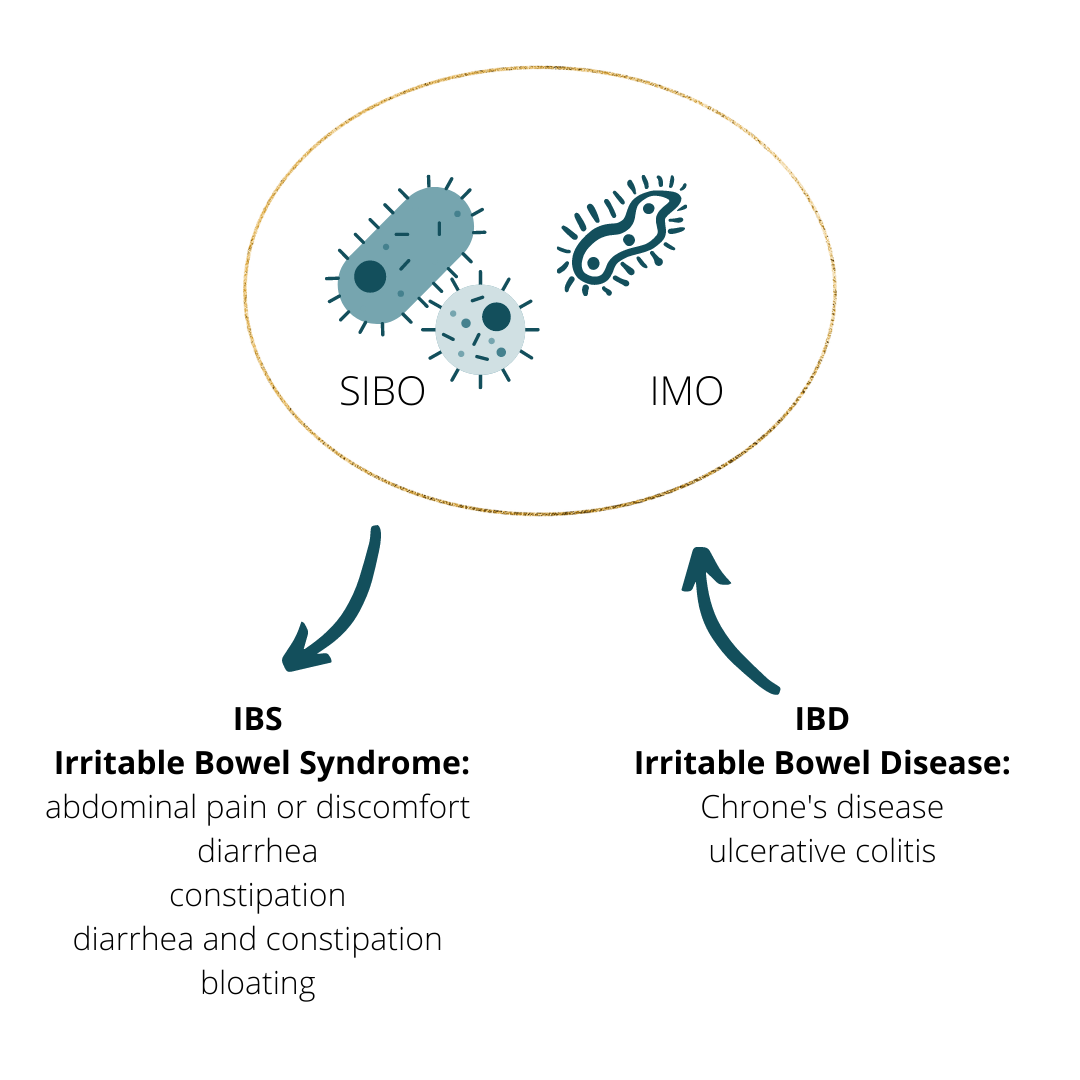
SIBO stands for Small Intestine Bacterial Overgrowth. SIBO and IMO, Intestine Methanogen Overgrowth, are both related to an overgrowth in the small intestine (instead of the large intestine which is where this stuff should live). Similar symptoms they share are abdominal bloating, pain, belching, and gas. How do they differ? SIBO produces excess hydrogen or hydrogen sulfide gas and causes diarrhea. IMO produces excess methane gas and causes constipation.
Symptoms of SIBO: similar to IBS
abdominal bloating and pain after eating⠀
Gas, belching
Diarrhea and/or constipation⠀
Brain fog/fatigue
Nausea
Food sensitivities and reactions
Poor nutrient absorption (B12, iron, etc.)
Diagnosis:
3-hour SIBO lactulose breath test. Trio smart is an at-home test that tests for hydrogen, methane, and hydrogen sulfide.
Treatment:
Antibiotics - Rifaximin (not absorbed, different than other antibiotics), antimicrobials (Allicin, Neem, Oragano), or elemental diet
It’s imperative to refer your patients to the right practitioner. Too often, if you send them to a random GI doc, they will tell them to “just eat more fiber” or that they just have constipation. Unfortunately, they are not likely to see significant improvement in their pelvic pain symptoms, which affects their ability to achieve their desired outcome with pelvic floor therapy.
We continue to lack solid research and still don’t know A LOT about gut health and how it is interconnected with the brain and chronic pain.
For now, connect with people in your local community for recommendations for GI, functional medicine, naturopaths, etc. Talk to local providers directly to get a better idea of what kind of care they can provide for your patients.
Specific to IC/painful bladder syndrome (PBS), as many as 40% – 60% of patients diagnosed with IBS also exhibit symptoms and fulfill diagnostic criteria for IC; correspondingly, 38% of patients diagnosed with IC also have symptoms and fulfill diagnostic criteria for IBS.
One meta-analysis provided epidemiological evidence of a link between endometriosis and IBS, highlighting two or more times higher risk of IBS in women with endometriosis compared to women without the condition.

Inflammatory bowel disease (IBD) is different from IBS, and Chron’s disease and ulcerative colitis fall under IBD. Although SIBO does not cause IBD, IBD can cause SIBO.
People can have IBS without SIBO, and although the evidence is limited, it’s clear there is a connection between IBS and pelvic pain. Also, those with IBS have a high occurrence of underlying SIBO.⠀
But wait, I’m not a GI doc or nutritionist - what can I do?
We all have a good understanding that chronic pain patients have a better outcome when they receive integrated care by a multidisciplinary team. Often as a pelvic health PT/OT, we are the leader of the “team” and we can’t expect patients to figure all of this out. By learning the basics we can educate our patients and refer them to those who will serve them best.
Possible Causes of SIBO:
Altered motility - slow transit, EDS
Endo, abdominal surgeries, cesarean birth - intra-abdominal adhesions
Leaky gut - excessive use of antibiotics, NSAIDS, etc.
Food poisoning
Opioids
Chronic constipation
Stress – decreased stomach acid, decreased production of digestive enzymes

Please share this with anyone whom you think would benefit from learning more about this - pelvic health PTs, OTs, medical providers, etc. Let’s get the word out!!
References:
Ayesha Shah, Nicholas J Talley, Mike Jones, Bradley J Kendall, Natasha Koloski, Marjorie M Walker, Mark Morrison, Gerald J Holtmann. Small Intestinal Bacterial Overgrowth in Irritable Bowel Syndrome: A Systemic Review and Meta-Analysis of Case-Control Studies. Am J Gastroenterol. 2020;115(2):190-201.
Chang, K.-M., Lee, M.-H., Lin, H.-H., Wu, S.-L., & Wu, H.-C. Does irritable bowel syndrome increase the risk of interstitial cystitis/bladder pain syndrome? A cohort study of long-term follow-up. International Urogynecology Journal. 2021;32(5), 1307–1312.
Leonard B Weinstock 1, Carl G Klutke, Henry C Lin. Small intestinal bacterial overgrowth in patients with interstitial cystitis and gastrointestinal symptoms. Dig Dis Sci. 2008;53(5):1246-51.
Francesca Chiaffarino, Sonia Cipriani, Elena Ricci, Paola Agnese Mauri, Giovanna Esposito, Marta Barretta, Paolo Vercellini, Fabio Parazzini. Endometriosis and irritable bowel syndrome: a systematic review and meta-analysis. Arch Gynecol Obstet. 2021;303(1):17-25.
Pimentel M, Saad RJ, Long MD, Rao SSC. ACG Clinical Guideline: Small Intestinal Bacterial Overgrowth. Am J Gastroenterol. 2020;115(2):165-178.
Sarna, Shivan. Healing SIBO. New York, Penguin Publishing Group, Kindle Edition, 2021.
Viganò D, Zara F, Usai P. Irritable bowel syndrome and endometriosis: New insights for old diseases. Digestive And Liver Disease: Official Journal Of The Italian Society Of Gastroenterology And The Italian Association For The Study Of The Liver. 2018;50(3):213-219.
Disclaimer: These self-care suggestions are for general use only and are not intended to be used as medical advice, diagnosis, or treatment. Refer to your medical provider for all questions and concerns regarding your individual care.