How to Help Stress Incontinence: A Pelvic Floor PT’s Guide to Understanding and Management
Pelvic floor physical therapy can help with stress urinary incontinence! Let's talk about solutions - how we can help. We cover what stress urinary incontinence is, causes and risk factors, bladder function, urinary system anatomy, treatment options, expectations, and outcomes.

Thanks to social media and people in the public being more comfortable talking about their bladder issues, stress urinary incontinence (SUI) is a problem that has received increased awareness over the past 5-10 years.
You may hear someone say “I laughed so hard I peed my pants” or hear a mom say that since she’s had kids, she has accidents with coughing or sneezing, or a group of moms joking about how they can’t jump on a trampoline anymore without leaking. Although this increased awareness is great, what we also need to be talking about are solutions - how to help stress incontinence.
In this blog post, we are going to cover:
What is stress urinary incontinence
Causes and risk factors
Bladder function basics
Anatomy review
Treatment options
Expectations and Outcomes
What is Stress Urinary Incontinence (SUI)?
Urinary incontinence (UI) simply means leaking urine. Incontinence can range from just a few drops to a full-blown bladder emptying, and it can range from annoying to embarrassing to radically limiting a person’s ability to exercise or interact in society.
Definition of stress urinary incontinence (SUI): involuntary leakage of urine during activities that put pressure on the bladder, such as coughing, sneezing, laughing, or exercise.
Stress urinary incontinence differes from urge urinary incontinence in that stress incontinence happens with an activity that increases intra-abdominal pressure on the bladder and urge incontinence is leakage with a sudden and strong urge to urinate. Urge incontinence is also associated with urinary frequency and urinary urgency (overactive bladder).
Due to the structure of the female urinary tract, as well as other effects from pregnancy, childbirth, and menopause, women are twice as likely as men to experience urinary incontinence. In a recent study of 5,006 women, 37.5% had stress urinary incontinence. While stress urinary incontinence can affect all people, this blog post is going to focus on the problem in people who have a vagina.
While stress urinary incontinence is common, that doesn’t mean that it’s “normal”.

Risk Factors for Stress Incontinence
Pregnancy
Vaginal childbirth
Aging (loss of muscle mass)
BMI more than or equal to 25
Chronic coughing
Pelvic surgery
Connective tissue disorders such as Ehlers-Danlos Syndrome (more on hypermobility and the pelvic floor)
Constipation
Prostate surgery
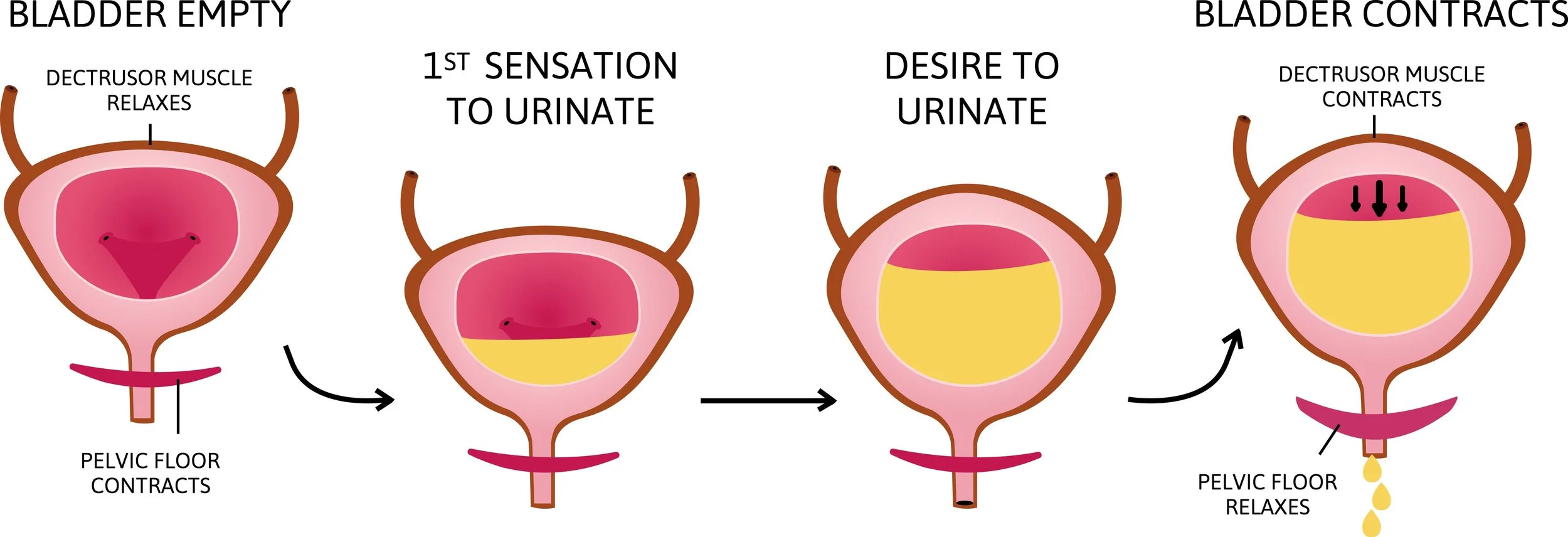
Bladder Function Basics
The term “stress urinary incontinence” is a symptom, and there can be different causes at play for different people. Learning about bladder function can be complicated, but let’s break this down:
The structures involved with bladder continence or leakage are: the bladder, urethra, urethral sphincter muscles, pelvic floor muscles, fascia, pudendal nerve, levator ani nerve, and intra-abdominal pressure. Everyone has a baseline resting closure pressure of the urethra, greater than the pressure in the bladder, when they have good functioning urethral sphincters (internal and external) and urethral vascularization. So, higher pressure closing the urethra, lower pressure from the bladder = we all stay dry.
When we urinate, we sit on the toilet, relax the urethral spincter and pelvic floor muscles, the bladder pressure is increased (because it is full) and contracts, and the pee comes out.
With laughing, jumping, coughing, or under load, the intra-abdominal pressure increases, transferring the pressure to the bladder. In a continent person, the load also transfers to the upper part of the urethra and increases urethral closing pressure, so they stay dry. This happens without conscious thought because that person has intact fascial function and intact and functional pelvic floor muscles.
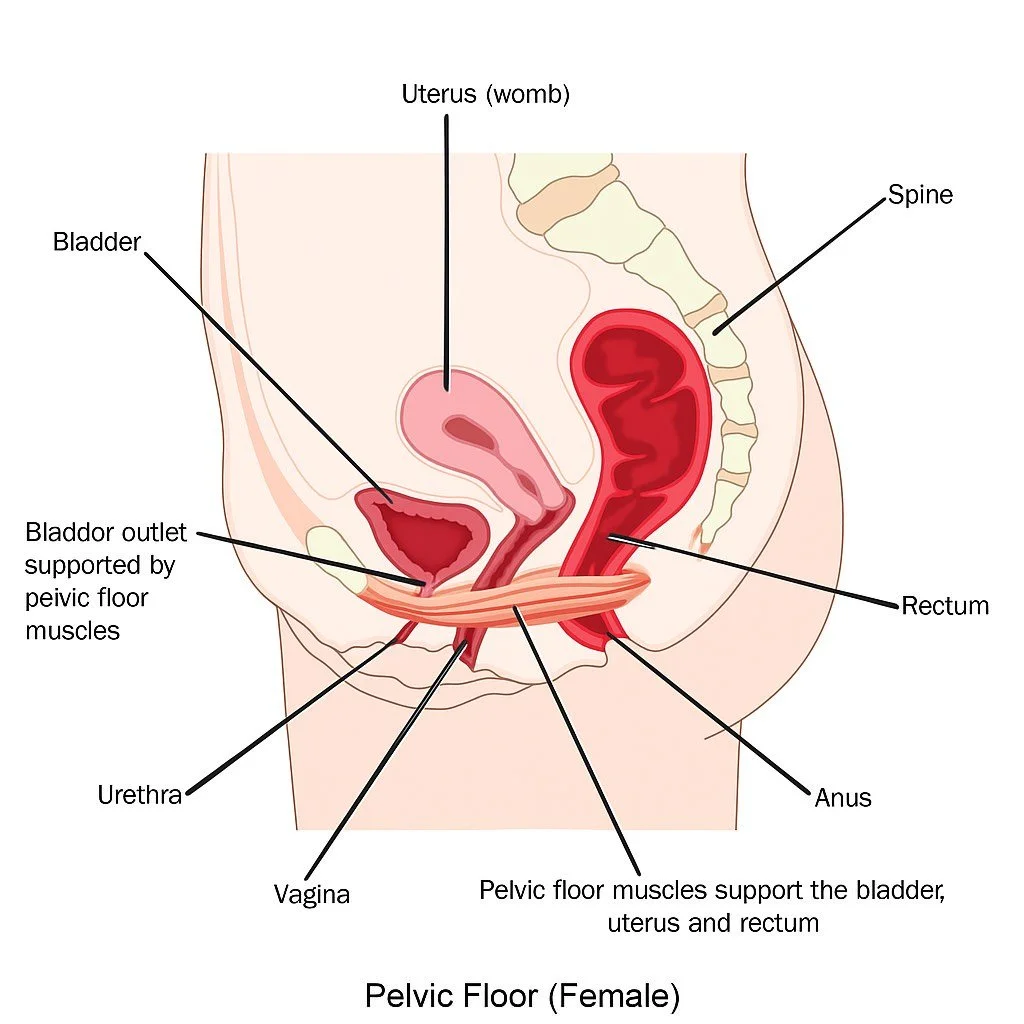
The Pelvic Floor Muscles and Fascia: Anatomy Review
The levator ani is a group of 3 muscles in the pelvic floor. They start at one side of the pubic ramus, wrap behind the rectum, and end on the other side of the pubic ramus. When doing a pelvic floor muscle contraction (a kegel), the muscles pull everything they are circled around (rectum, vagina, urethra) forward.
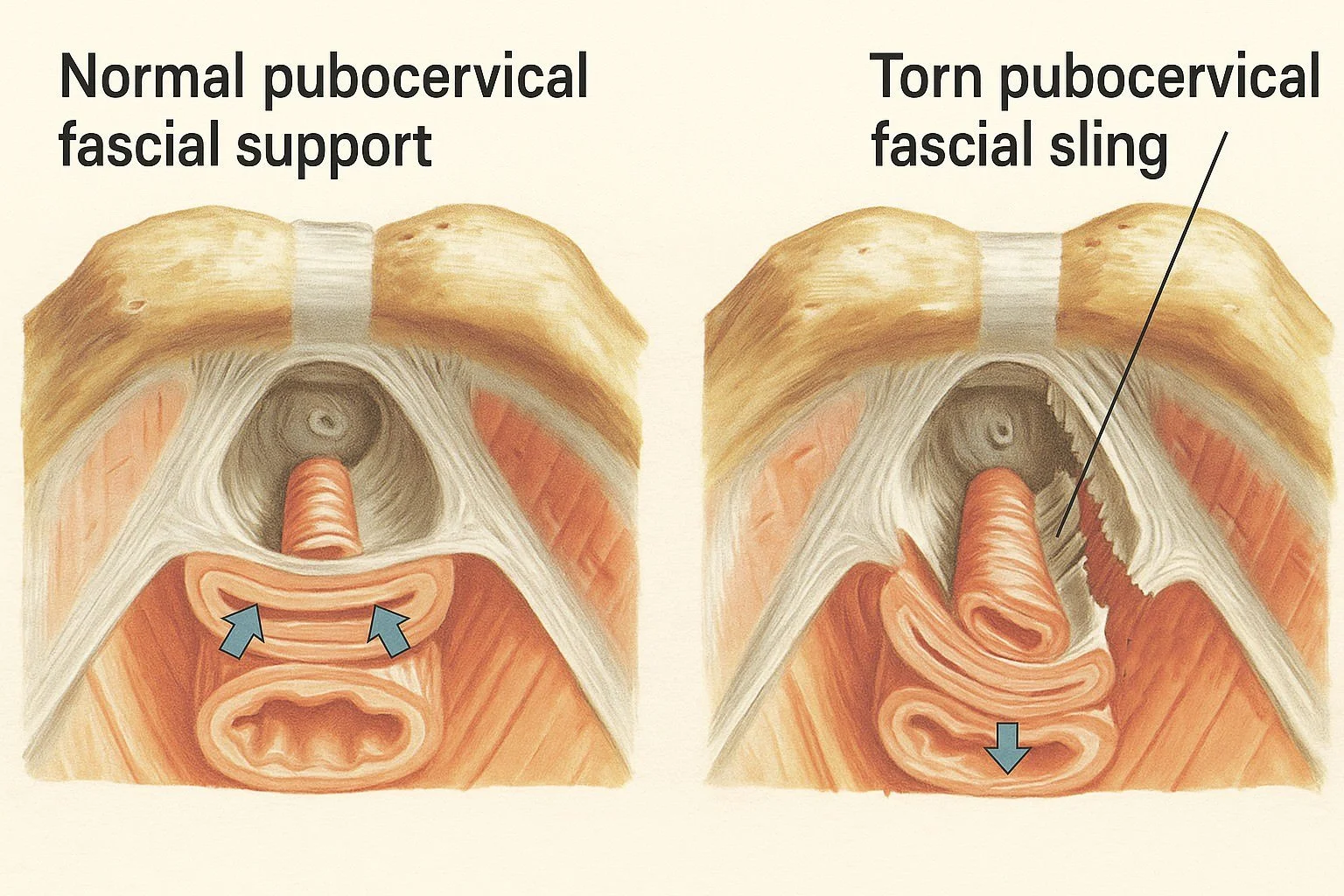
They don’t circle around the urethra, so they can’t directly increase urethral pressure on their own. However, the pubocervical fascia lies between the back part of the bladder and urethra and the front wall of the vagina. The levator ani is attached to this fascia on the sides, so that when the levator ani contracts, it pulls the fascia forward, and as the fascia pulls taut, it elevates the bladder neck and urethra. Now, when there is increased abdominal pressure, this pressure pushes the urethra from the front against a firm backdrop (the pubocervical fascia) and increases the urethral closure = no leaking.
If the pubocervical fascia is damaged from vaginal childbirth, it can’t provide that firm backdrop, leading to urethral hypermobility, and can contribute to urinary leakage.
Because of the risk factors mentioned above (vaginal birth, constipation, age-related muscle loss, etc.), not everyone has intact fascial function, functional pelvic floor muscles, and strong urethral sphincter muscles to withstand the amount of pressure generated throughout the day. So they leak.
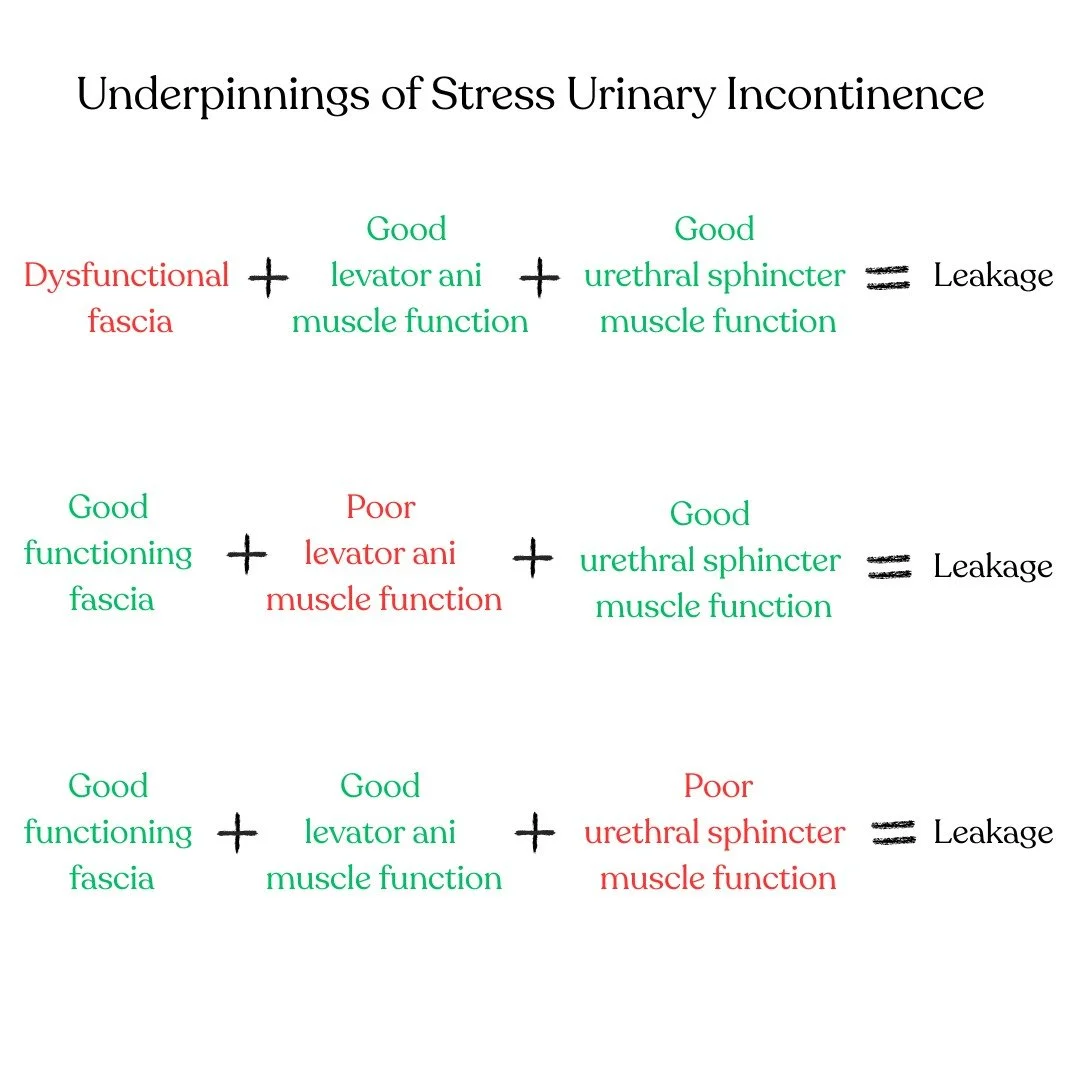
To summarize: we need strong, coordinated pelvic floor muscles (levator ani), intact pubocervical fascia, and strong urethral spincter muscles.
In fact, we now believe the urethral sphincter muscles may have more of an impact on continence than the levator ani muscles. In a study by Falah-Hassani et al in 2021, they found that the women with stress urinary incontinence had thinner and smaller urethral sphincter muscles, had a shorter urethra, and slower nerve function of the perineal branch of the pudendal nerve (which innervates the external urethral sphincter).
Now that we know the causes of stress urinary incontinence, what can we do about it?
Treatment Options: Pelvic Floor Physical Therapy
An initial visit with a pelvic floor physical therapist may involve:
Medical and bladder history
Posture and breathing assessment
Movement and strength assessment
Internal pelvic exam (if appropriate and consented)
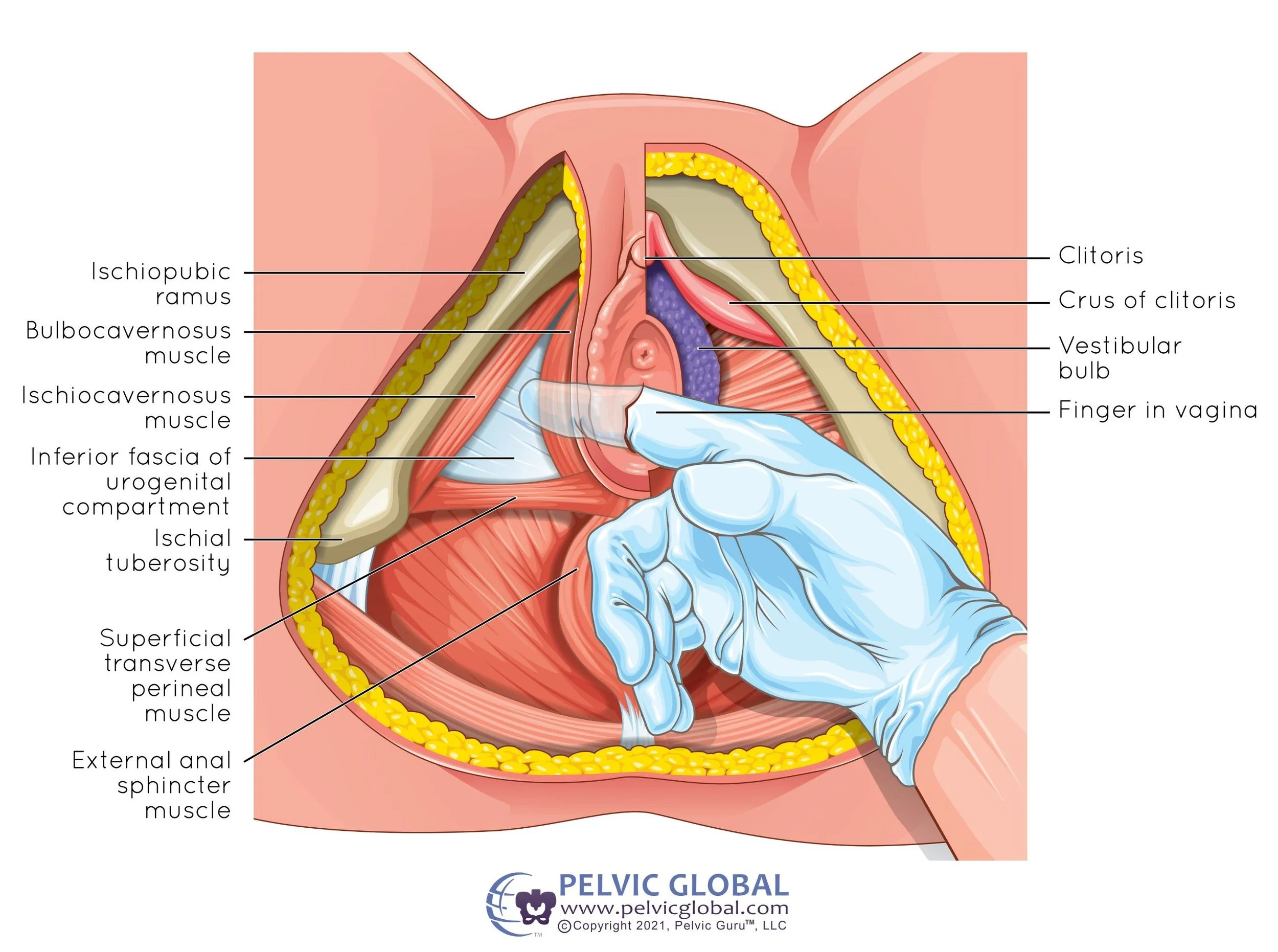
Let’s talk more about the internal (vaginal) pelvic exam. Clinically, we do this with a gloved finger inserted in the vagia and assess pelvic floor muscle tone, discomfort with pressure, and muscle function. With muscle function, we are aiming to assess a person’s strength, endurance, contraction quality, accessory muscle use, and ability to relax the muscles.
When assessing muscle contraction, we believe that these cues target the anal sphincter and levator ani muscles of the pelvic floor:
Close your anus as if you’re trying to prevent passing gas
Pretend you’re holding a marble inside your vagina and you don’t want it to fall out
Pick up a blueberry with your vagina
Pull my finger up and in (with a finger inserted in the vagina)
While these cues may target more of the urethral sphincter muscles:
Stop the pee flow
Think of closing your labia together like butterfly wings
Pull your clitoral hood down
Nod or pull down your clitoris
Knowing that all three areas, good levator ani muscle function, good urethral sphincter muscle function, and good functioning fascia, play a role in continence, is there a way to assess intact fascia? While this can be assessed with real-time ultrasound, most PTs in the US don’t have access to this, so it is underutilized. However, we can still create a treatment plan based on the information we are able to gather.
Where do we start?
Pelvic Floor Muscle Training (kegels)
While the average “cure” rate (no more leakage) of stress urinary incontinence with pelvic floor muscle training is 51-56%, it is believed that improvement in this area is a good first start.
According to the 7th International Consultation on Incontinence in 2023, “Supervised pelvic floor muscle training should be offered as first-line conservative therapy for women of all ages with urinary incontinence.” Additionally, the NICE Guidelines from 2019 suggest “clinicians should offer a supervised pelvic floor muscle training of at least 3 months duration as first-line treatment to females with SUI.”
Things to consider with pelvic floor muscle training:
-Cuing: levator ani muscles, urethral sphincter muscles, or both?
-Teach people to do a pelvic floor muscle contraction when they are about to cough, sneeze, or lift something heavy (called “the knack”).
-Frequency and duration to improve coordination and muscle hypertrophy
Pelvic floor muscles are composed of 70% slow-twitch and 30% fast-twitch fibers. Long-standing research shows that 3 sets of 8-12 maximal contractions, 3-4x/week for 8-12 weeks, leads to improved strength and muscle thickness.
Sustained contractions of 6-10 seconds with full relaxation in between are most effective.
Rest 6-10 seconds between repetitions and 30-60 seconds in between sets.
As the fast-twitch fibers are more likely to have an impact during quick contractions, like with coughing or jumping, it makes sense to promote hypertrophy in primarily these fibers by adding 5-10 rapid contractions (called “quick flicks”) at the end of each set.
Other Areas of Pelvic Floor PT - it’s more than kegels!
Here are some other areas that we can address that may impact leakage:
-Posture: excessive anterior pelvic tilt, rib flaring, abdominal clenching, or excessive slumping
-Breathing: shallow breathing, breath holding, tightness in ribs and middle spine
-Strength and endurance of pelvic floor accessory muscles - abdominals, outer hips, inner thighs, glutes
-Manual therapy: Due to the attachment of the levator ani muscles to the obturator internus muscle via the arcus tendineus, increased tone in the levator ani muscles results in increased tone in the obturator internus muscles.
Because increased tone in the obturator internus can compress the perineal branch of the pudendal nerve, which also innervates the external urethral sphincter, doing manual therapy (trigger point release, stretching, massage, pelvic wand) can relieve this compression, allowing the nerve and external urethral sphincter to function better.
-Consider compound movements and accessory muscle use to progressively challenge the muscles. For example:
Adding a pelvic floor muscle contraction with any exercise, such as a squat, bridge, or jump
Squeezing a ball between your knees or using a resistance band loop above your knees during dynamic exercises for accessory muscle assist
Coordinating breath with movement
Progression options: increased resistance, supine to upright, increased speed, etc.
With all exercises, we encourage the number of repetitions and difficulty to be below the threshold of leakage.
Other Treatment Options
External devices: can be fantastic for those with fascial disruption or who don’t see improvement with the above treatment options
Revive: a reusable device that provides temporary support to the urethra. It's a one-size-fits-most silicone pessary that is inserted internally.
Poise Impressa: a single-use, over-the-counter device, similar to a tampon, that is inserted into the vaginal canal to provide support to the bladder and urethra.
Pessary: a reusable device, fitted by a medical professional, to lift the bladder to help reduce or eliminate leakage.
Medical: rate of improvement, risk factors, and rate of relapse are beyond the scope of this blog
Bulkamid injection: a minimally invasive procedure that involves injecting a hydrogel called Bulkamid into the urethral wall to add bulk and support the urethra, helping to prevent urine leakage during activities that increase abdominal pressure, like coughing or sneezing.
Transvaginal Tape (TVT): a surgical procedure in which a mesh tape is placed behind the urethra through a vaginal incision and then passed behind the pubic bone to exit through small abdominal incisions. Provides support to the urethra and bladder neck, preventing leakage during activities that increase abdominal pressure. Associated risks: bladder perforation and groin pain.
Bladder Sling Procedure: a surgical procedure involving placing the mesh through the obturator foramen (transobturator tape or TOT). Fewer incisions, but may not be as effective for severe SUI.
Expectations and Outcomes
I typically tell people to expect improvement in their symptoms in 3-6 months, but there is no set timeline, as it depends on the severity of symptoms, the structures involved (muscles vs. fascia), the frequency and consistency of the person working on the problem, etc.
We also can’t directly compare the success rates of pelvic floor physical therapy with other interventions because pelvic floor physical therapy and stress incontinence research primarily study pelvic floor muscle training, which is significantly limited.
As mentioned above, there is so much more to pelvic floor physical therapy than just kegels! Although there is a great need for more diversified research that covers what we actually do in the clinic, I can say that pelvic floor physical therapy is a less invasive and highly successful way to approach and treat stress urinary incontinence.
Hopefully, after reading this blog, you have gained insight about how to help stress incontinence, and you no longer think:
“Kegels are the only solution.”
“It’s just part of getting older.”
“Surgery is the only option.”
If you’re struggling with bladder leakage and you live in fear of having an accident or limit your activity to avoid embarrassment, you’re not alone! I hope this blog helped you gain insight into how to help stress incontinence.
I encourage anyone with this issue to find a qualified pelvic floor physical therapist in their area and get started on an action plan. If you live in the greater Minneapolis, MN area, schedule a consult with me or reach out to me if you have questions!
Did you like this blog? Here’s what’s next on your reading list:
Disclaimer: The information in this blog post is for general purposes only and is not intended to be used as medical advice, diagnosis, or treatment. Refer to your medical provider for all questions and concerns regarding your individual care.
Quick self-check
Curious if you might have pelvic floor dysfunction?
Take this quick self-screen. 10 yes/no questions, about a minute. Your answers stay on your device.
Did you enjoy this post? Whether you're a newbie or a pelvic pro, join the community to stay up to date with the latest and greatest in pelvic health!