What to Do For Diastasis Recti: A Pelvic Floor PT’s Perspective
If you’ve been told never to do planks or crunches postpartum - you’re not alone! Many myths about diastasis recti, or diastasis rectus abdominis (DRA), continue to circulate. We aim to answer the most common questions about diastasis recti and clear up misconceptions. This includes reviewing research consensus and our beliefs, which are based on theory and clinical experience (because, spoiler alert, evidence about all things DRA is pretty weak!). We are going to cover:
What exactly IS diastasis recti, and how is it diagnosed
How common is diastasis recti, what causes it, and what does it look like
What are the most common concerns about diastasis recti
Myths and misconceptions about diastasis recti
How to treat and manage diastasis recti
What is doming/coning during exercise or activity, and is it “bad”
What are some principles I find helpful
Key Takeaways
Diastasis recti is a normal and common change in pregnancy.
The “gap” alone does not determine function or symptoms.
Exercise does not make DRA worse - and is helpful.
Doming is not automatically bad.
Treatment should focus on strength, confidence, and functional goals - not chase a perfect gap width
What exactly IS Diastasis Recti
First, let’s review what diastasis recti is and what it isn't. Diastasis Rectus Abdominis is defined as “an impairment with midline separation of the two rectus abdominis muscles along the linea alba” (Bo et al, 2017). It is a separation or stretching of the linea alba in the midline of the abdomen. The linea alba is located between the rectus abdominis and has connections to the rectus abdominis, transversus abdominis, internal, and external oblique abdominal muscles. It is composed of connective tissue and adapts to load and increased tension to transmit forces.
Diastasis recti is not a tear or a hernia, and it is not an injury, so it doesn’t need to “heal”.
Because the linea alba is made up of tissue connected to other muscles and fascia, its function can change, and it’s not a fixed entity.

How is it diagnosed?
How is a diastasis recti assessed? One way is to measure the inter-recti distance (the distance between the 2 medial edges of the rectus abdominis muscle). The accuracy of measurement depends on the method - palpation with fingers, caliper, or ultrasound. Ultrasound is the most accurate method (Chmielewska et al. 2024); however, most PTs in the US do not have access to ultrasound in their clinics.
There is no universal definition of how much separation is “normal”. It is normal to have some separation after pregnancy, and it is more common to have more separation above the umbilicus than below. Diastasis recti has been defined as “a separation of >2.2cm at 3cm above the umbilicus”(Beer et al. 2009). But is the >2.2cm measurement meaningful? A study by Kaufmann et al. (2022) showed that a lot of asymptomatic people had up to a 3.4cm separation (3cm above the umbilicus), so the definition of what is considered a “problem” is a bit hazy. Additionally, some people can have a wider DRA without issues, and some can have a narrow separation with more issues. We’ll talk more about the “issues” with DRA later on, so keep this in mind!
How common is DRA?
Based on inter-recti distance measurements postpartum, the incidence is 60% at week 6, 45% at 6 months, 33% at 12 months postpartum, and seems to decrease with age (Sperstad et al, 2016). Again, these numbers can vary depending on the measurement method and the measurements used to define a diastasis recti.
So far, we don’t have consistent ways to measure a diastasis recti, and we don’t have a clear definition of how much separation is a “problem”. Still with me? Let’s keep going!
What causes diastasis recti?
Why does this separation happen? It can happen to people at any point in their lives, across all genders, and even in kids, but it is most common during the perinatal period. This makes sense - the tissues stretch to make room for the growing baby, and studies show that between 67-100% of pregnant people have a diastasis recti during their third trimester (Boissonnault et al, 1988). So, anyone selling you something that says it can “prevent” a DRA during pregnancy is a bunch of BS.
Risk factors include:
an increasing number of pregnancies
cesarean birth if more than 2 births
higher BMI
diabetes
By the way, it’s not just the linea alba that stretches. Any of the following can be impacted:
rectus abdominis
external oblique
internal oblique
transversus abdominis
diaphragm
linea alba
sheaths (rectus abdominis, external oblique, internal oblique, transversus abdominis)
thoracolumbar fascia
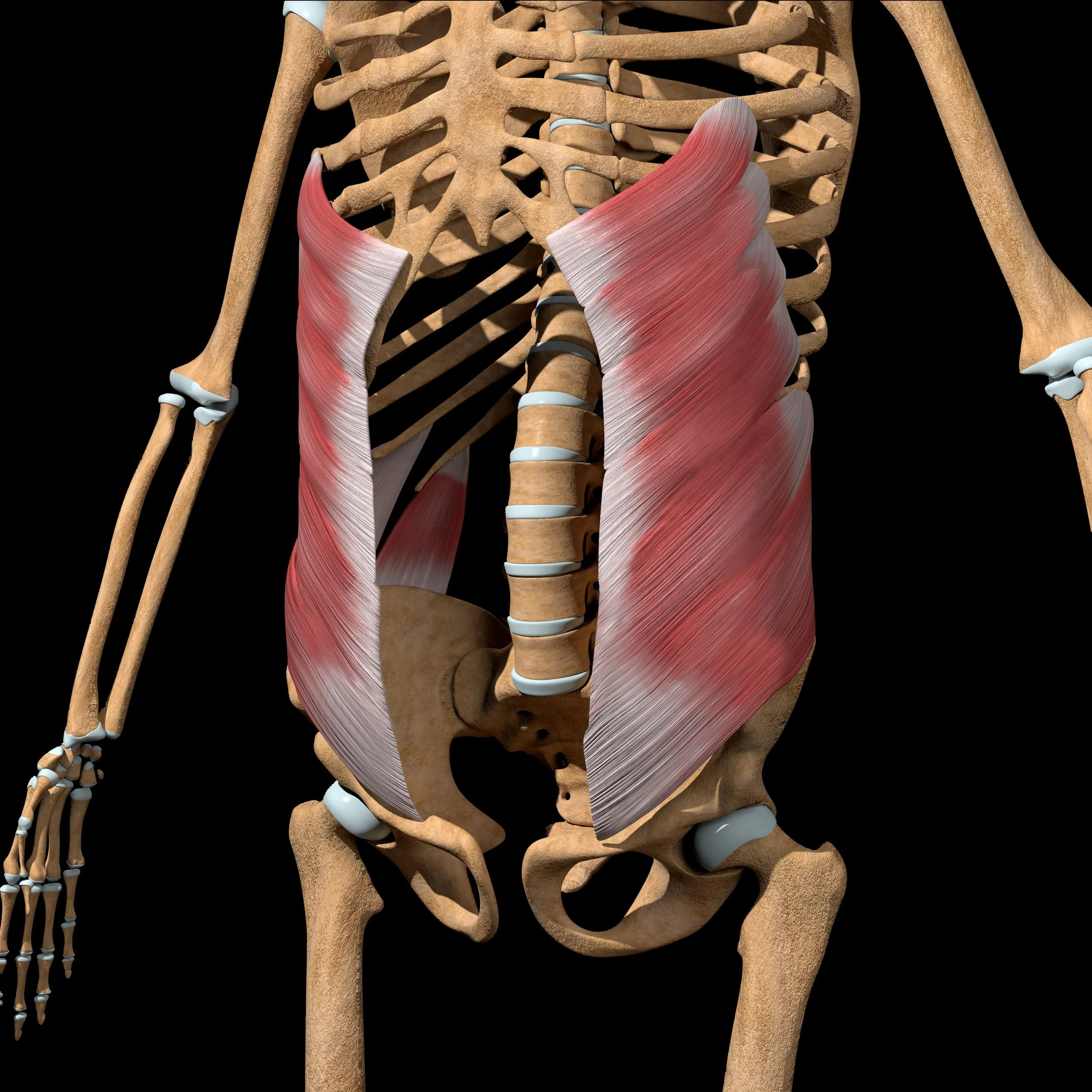




Recovery of all abdominal muscles can impact function.

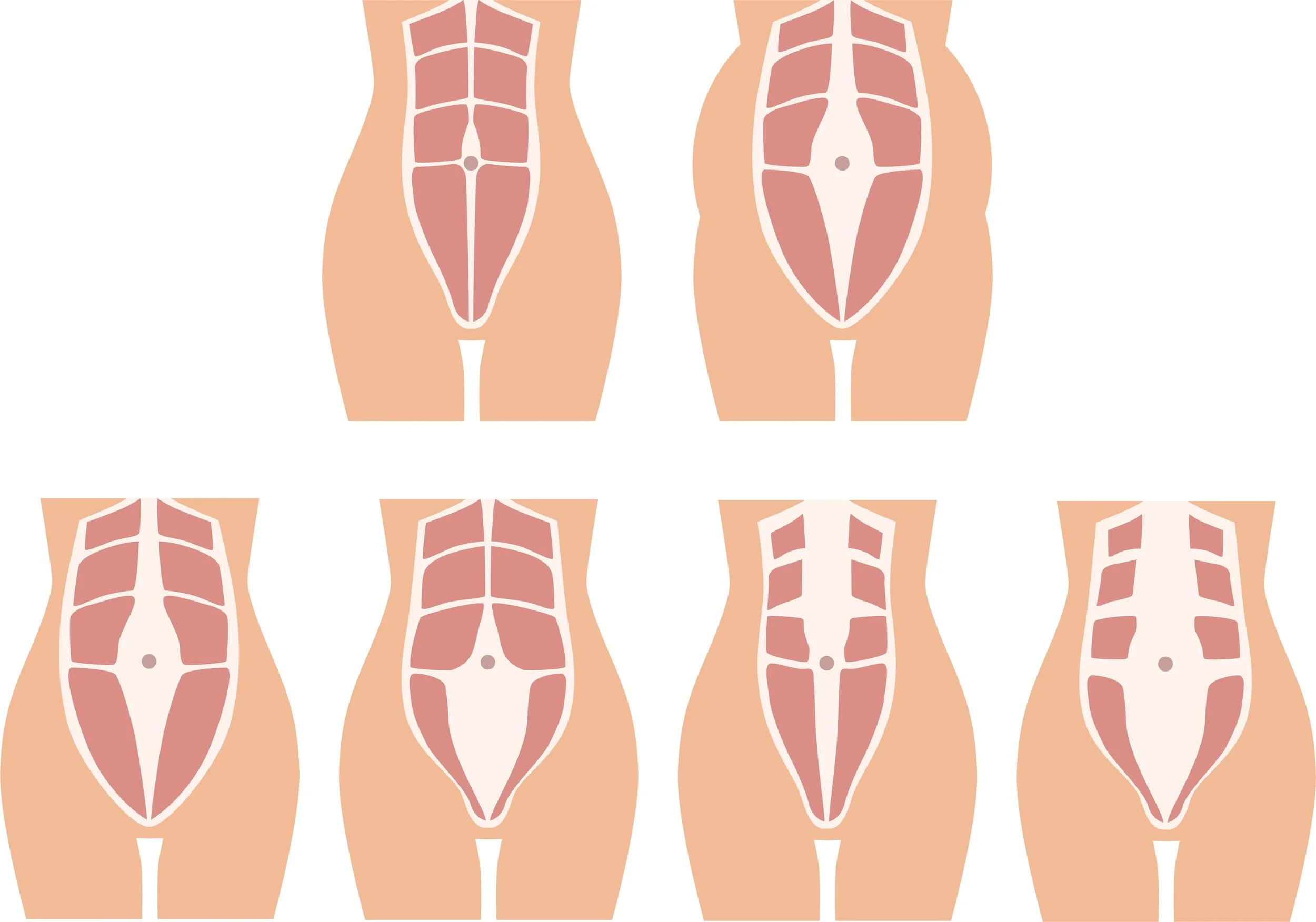
What does diastasis recti look like?
It depends. During pregnancy, especially the 3rd trimester, this can look like a vertical triangle or dome in the middle of the belly during an effortful movement such as getting into bed, rolling over in bed, doing an abdominal crunch, sitting up in bed, or any core exercise. It can also look this way postpartum, or it can look like a shallow divot, or concave hole, in the middle of their abdomen, or an overall protruding belly.
The problem with belly protrusion: these are the people who report that strangers ask them “when you are due” after already giving birth. (Btw, people need to stop saying this! No one wants to look or feel pregnant after giving birth, and it can be very hurtful, so unless you know the person, and you are 100% positive they are still pregnant, don’t ask this!)
Myths and misconceptions about diastasis recti
🚫DRA causes problems like low back pain and pelvic floor problems. False
There is no direct correlation according to current research. (Gluppe et al., 2021, Fei et al., 2021). There is some low-quality evidence that DRA severity is associated with low back pain (Benjamin et al, 2019), but unclear if the correlation is due to the presence of a DRA or limitations in activity and exercise due to fear of making the DRA “worse” (leading to increased inactivity and loss of muscle mass).
🚫Doing planks, crunches, or any exercises on hands and knees will make your DRA worse. False.
Exercise has not been shown in the research to make a DRA worse. We do know that the rectus abdominis contraction can narrow the inter-recti distance (Lee and Hodges, 2016) and, due to its attachments to the external obliques, internal obliques, transversus abdominis, and linea alba, hypertrophy of the rectus abdominis may improve the tension in the linea alba, therefore improving its function and overall appearance. While we do express caution with “doming” while exercising if a person is pregnant or postpartum (more on “doming” later!), no studies are showing specific exercises to be “good” or “bad” for someone with a DRA.
🚫Does wearing a belly band or abdominal brace postpartum help? Yes and no. No, it hasn’t been shown to reduce DRA width (Depledge et al. 2023); however, especially after a cesarean birth, people may feel better with activity while wearing a support brace for up to 8 weeks postpartum. Since we know that recovery and strength gains are improved with movement and activity, it makes sense to help people optimize this postpartum.
On a personal note, I did wear an abdominal brace/belly band for the first 2 months after my twin cesarean birth. I had way less discomfort with bed mobility, transfers, and just basic movement while caring for my new babies. So, this was a huge help to me, but each person can decide for themselves what feels good for them during their early postpartum recovery.
What are the most common concerns about diastasis recti? (aka, why is diastasis recti a “problem”?)
These are the most common concerns I hear, in regards to DRA:
They don’t like how their belly looks
They don’t like how their abdomen feels with activity or exercise
“I look like I’m still pregnant.”
“I can’t feel my core working at all!”
Keep in mind: stretched skin can only rebound so much, a layer of abdominal fat will impact how the belly looks, and having more muscle can help the appearance of tissue tautness. Example: someone with saggy skin and tissue at the back of their upper arm may improve the appearance by building up the upper arm muscles, making the skin more taut and appearing less saggy. The same can be applied to stretched-out abdominal skin and the muscles underneath, to a certain extent. Beefier muscles take up more tension in skin and fascia.
What does a pelvic floor physical therapy assessment look like?
Here are some of the areas I look at and work on with people during pregnancy and postpartum recovery:
✅Posture, rib/pelvis alignment, breathing, and standing abdominal assessment
✅Stability tests, abdominal challenges, and abdominal palpation
✅Transversus abdominis and pelvic floor muscle activation
✅DRA assessment: length, width at rest, width change with various exercises and cuing, depth of gap, doming/tenting/coning
✅Abdominal assessment with exercise and movement in all positions
I observe how things look, feel, and task difficulty, and find out how they feel. This gives me an idea of where the person is starting from, so we can build an appropriate program.
How to treat and manage diastasis recti
The path is nuanced. Comparing research is limited due to different methods used, and most studies have low-quality evidence to support their efficacy.
There isn’t a clear definition of what “fixed” looks like.
Goals can vary, such as: a decrease in abdominal circumference, less “doming” with movement and exercise, feeling stronger in their core with activity, etc. Research doesn’t provide concrete ways to “close the gap,” and “closing the gap” may not lead to any meaningful changes.
What do we know?
Time = recovery: Spontaneous improvement is the greatest during the first 12 weeks postpartum but continues throughout the first year.
Exercise is helpful! (Weingerl et al. 2023). Specific exercises have low-quality evidence supporting their efficacy at this time (Weingerl et al., 2023; Benjamin et al., 2023). However, clinically, we find that improvements in abdominal strength, endurance, and muscle hypertrophy can improve overall appearance and confidence during exercise and daily activities.
Other interventions may be helpful, such as manual therapy, trigger point release, cesarean or abdominal scar tissue work, taping, electrotherapy, acupuncture, etc., but all have low-quality evidence supporting their efficacy at this time (Weingerl et al. 2023, Benjamin et al. 2023).
Surgery: DRA correction, with or without abdominoplasty. Risk factors include post-op complications such as seroma formation, wound infection, pain, numbness, time off for recovery, etc.

A word about surgery: Non-invasive interventions are limited, and tissue can be stretched beyond the point at which a person can achieve their aesthetic or functional goals, so we need to approach this without judgment.
Surgically fixing the abdominal wall appearance and/or function is not an “easy-out”.
What is doming/coning during exercise?
This is seen as a vertical bulge in the midline of the abdomen caused by a lack of tension at the linea alba during a movement or activity, such as sitting up to get out of bed. It can look rounded, like a dome, or triangular-shaped. The protrusion is caused by a load (intra-abdominal pressure), pushing the internal abdominal contents forward, that surpasses the ability of the abdomen to maintain enough tension. This is caused by a stretched-out linea alba and a lack of tension from all surrounding structures: abdominal muscles, fascia, diaphragm, pelvic floor muscles, etc.
If I see “doming” or “coning” during exercise, is that “bad” or will it make my DRA worse?
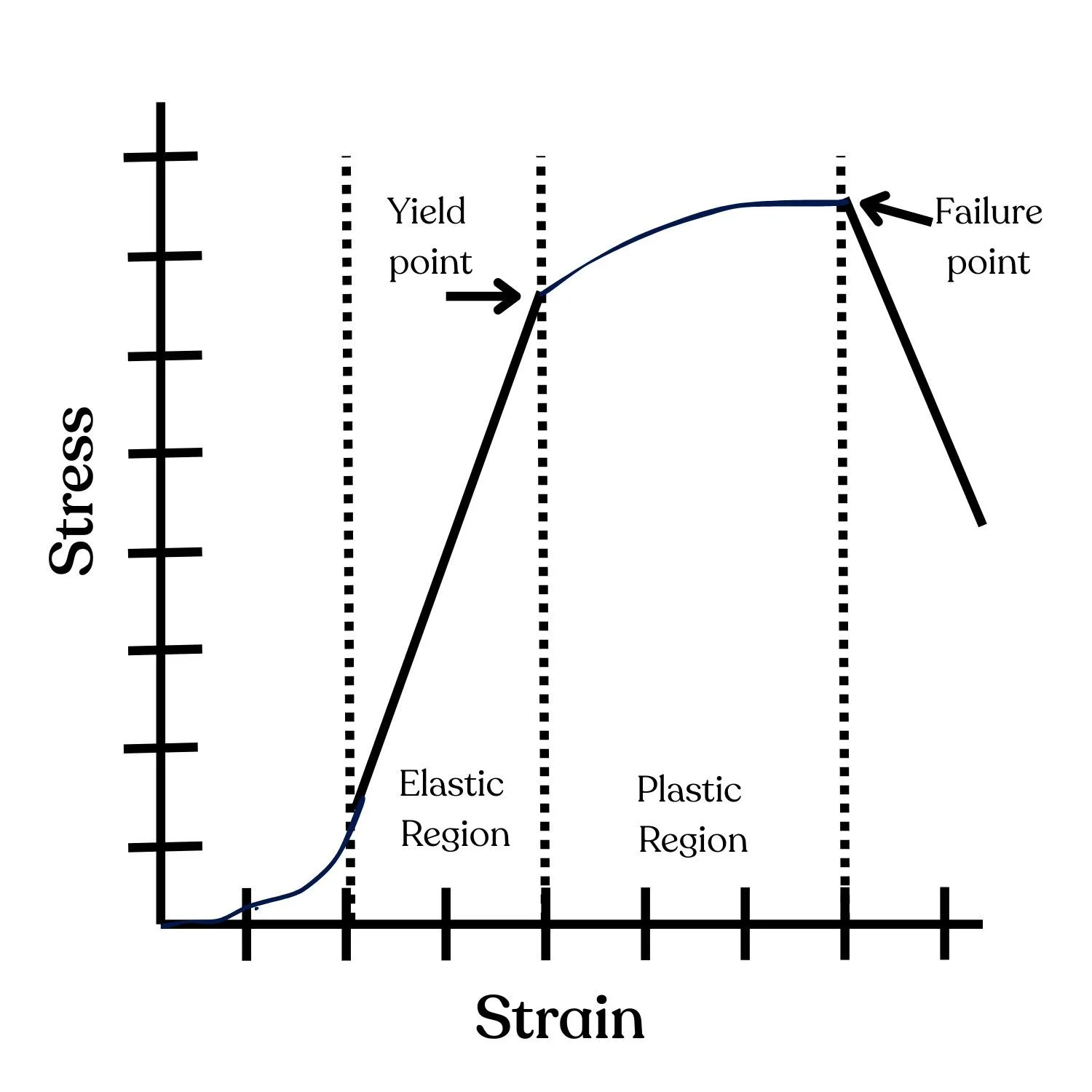
Tension is needed to stimulate adaptation (muscle strength, endurance, hypertrophy), so the goal with exercise is to keep the tension at levels that promote positive adaptation without negative consequences. All tissue has a tension limit, so we want to keep that limit under the threshold of tissue damage.
Current experts postulate that “soft doming” during exercise is not harmful because the pressure exerted is considered in the “elastic region” and unlikely to cause tissue damage or make the DRA worse. “Hard doming” may signal excessive load and be better avoided as the pressure exerted is considered more in the “plastic region”, and could potentially cause tissue damage.
If there is a “dome”, how can we check to see if it’s hard or soft? When someone does a movement that causes doming, we can press down firmly at the midline, just above the umbilicus. With a “soft dome,” the umbilicus feels soft; you can push down at the middle, and you can feel the edges of the rectus abdominis muscles on either side. A “hard dome” feels hard at the belly button, and you can’t feel the edges of the rectus abdominis muscle - it all feels hard.
What can we do if there is “hard doming”?
Lots of things! There are many ways to perform an exercise or activity that can result in changes in intra-abdominal pressure and tension. Here are some options:
💡Change breathing techniques: breath holding, exhale, inhale, rib expansion breathing (rather than “belly breathing”), etc.
💡Muscle contraction before and during a movement or an exercise (or not!): pelvic floor muscles, abdominal draw-in maneuver, transversus abdominis, etc.
💡Other changes you can make:
exercise difficulty
simple vs. complex movement
range of motion
posture or technique with exercise
amount of load or speed
location of exercise (example: planks off a bench vs on the floor)
impact
fatiguability: sets, reps
directional motion (sagittal, coronal, transverse plane, or combo).
A note about pressure: Any activity that causes a muscular contraction of the trunk muscles will increase intra-abdominal pressure. For those with DRA, it’s important to coach people not to “bear down” or “strain” into their pelvic floor. This can cause pressure management problems in the pelvic floor (aka, pelvic organ prolapse), which would not be ideal.
What are some principles I find helpful:

In general, life is not a series of fixed, controlled movements, so we need to train people to have resilience and adaptability with a variety of activities and exercises to facilitate success in real life.
✅Start with more basic, simple exercises, and then progress to complex ones with increased load. Postpartum people have to lift, carry, and even have their kids jump into their arms - we need to be training them accordingly.
✅Focus on their goals - aesthetic, exercise, movement, activities, etc. If someone needs to start at a lower level, we need to offer modifications, assure them that it’s temporary, and reinforce their long-term goals.
✅Limit fear. Our narrative matters: we need to have caution when we tell someone that their muscles are “weak” or when we excessively limit their activity and exercise, which can be harmful. We need to find ways to instill confidence that our patients are strong, capable, adaptable, and resilient (from Antony Lo's course, “Diastasis Done Differently”).

In Summary:
Research on diagnosis and treatment of DRA is weak because there are inconsistent ways to define it, measure it, and the results of interventions (“narrowing the gap”) may not may not impact a person’s goals or quality of life.
We need to take a nuanced approach when working with people with diastasis recti and offer individualized treatment plans that focus on building confidence in their current abilities with progression toward future goals.
I hope this blog helped you gain insight about diastasis recti: what we know, what we don’t know, and what can be done for it. If you’re unsure where to start or feel stuck with your progress, I’d love to help. I offer individualized assessments and strength-based treatments to help you return to the activities you love. 💛💛💛
If you live in the greater Minneapolis, MN area, schedule a consult with me or reach out if you have questions.
References:
Bø K, Hilde G, Tennfjord MK, Sperstad JB, Engh ME. Pelvic floor muscle function, pelvic floor dysfunction and diastasis recti abdominis: Prospective cohort study. Neurourol Urodyn. 2017 Mar;36(3):716-721. doi: 10.1002/nau.23005. Epub 2016 Mar 31. PMID: 27037746.
Chmielewska, D., Cebula, M., Gnat, R., Rudek-Zeprzałka, M., Gruszczyńska, K., Baron, J., & Opala-Berdzik, A. (2024). Reliability of inter-recti distance measurement on ultrasound images captured by novice examiners. Physiotherapy Theory and Practice, 40(11), 2652–2660. https://doi.org/10.1080/09593985.2023.2255897
Beer, G. M., Schuster, A., Seifert, B., Manestar, M., Mihic-Probst, D., & Weber, S. A. (2009). The normal width of the linea alba in nulliparous women. Clinical Anatomy, 22(6), 706–711. https://doi.org/10.1002/ca.20836
Kaufmann, R. L., Reiner, C. S., Dietz, U. A., Clavien, P. A., Vonlanthen, R., & Käser, S. A. (2022). Normal width of the linea alba, prevalence, and risk factors for diastasis recti abdominis in adults, a cross-sectional study. Hernia : The Journal of Hernias and Abdominal Wall Surgery, 26(2), 609–618. https://doi.org/10.1007/s10029-021-02493-7
Sperstad JB, Tennfjord MK, Hilde G, Ellström-Engh M, Bø K. Diastasis recti abdominis during pregnancy and 12 months after childbirth: prevalence, risk factors and report of lumbopelvic pain. Br J Sports Med. 2016 Sep;50(17):1092-6. doi: 10.1136/bjsports-2016-096065. Epub 2016 Jun 20. PMID: 27324871; PMCID: PMC5013086.
Boissonnault, J. S., & Blaschak, M. J. (1988). Incidence of Diastasis Recti Abdominis During the Childbearing Year. Physical Therapy, 68(7), 1082–1086. https://doi.org/10.1093/ptj/68.7.1082
Gluppe, S., Ellström Engh, M., & Kari, B. (2021). Women with diastasis recti abdominis might have weaker abdominal muscles and more abdominal pain, but no higher prevalence of pelvic floor disorders, low back and pelvic girdle pain than women without diastasis recti abdominis. Physiotherapy, 111, 57–65. https://doi.org/10.1016/j.physio.2021.01.008
Fei H, Liu Y, Li M, He J, Liu L, Li J, Wan Y, Li T. The relationship of severity in diastasis recti abdominis and pelvic floor dysfunction: a retrospective cohort study. BMC Womens Health. 2021 Feb 15;21(1):68. doi: 10.1186/s12905-021-01194-8. PMID: 33588826; PMCID: PMC7885475.
Benjamin, D. R., Frawley, H. C., Shields, N., van de Water, A. T. M., & Taylor, N. F. (2019). Relationship between diastasis of the rectus abdominis muscle (DRAM) and musculoskeletal dysfunctions, pain and quality of life: a systematic review. Physiotherapy, 105(1), 24–34. https://doi.org/10.1016/j.physio.2018.07.002
Lee, D., & Hodges, P. W. (2016). Behavior of the Linea Alba During a Curl-up Task in Diastasis Rectus Abdominis: An Observational Study. The Journal of Orthopaedic and Sports Physical Therapy, 46(7), 580–589. https://doi.org/10.2519/jospt.2016.6536
Depledge, J., McNair, P., & Ellis, R. (2022). The effect of Tubigrip and a rigid belt on rectus abdominus diastasis immediately postpartum: A randomised clinical trial. Musculoskeletal Science & Practice, June, 102712. https://doi.org/10.1016/j.msksp.2022.102712
Weingerl, I., Kozinc, Ž., & Šarabon, N. (2023). The Effects of Conservative Interventions for treating Diastasis Recti Abdominis in Postpartum Women: a Review with Meta-analysis. SN Comprehensive Clinical Medicine, 5(1), 10. https://doi.org/10.1007/s42399-022-01353-4
Benjamin, D. R., Frawley, H. C., Shields, N., Peiris, C. L., van de Water, A. T. M., Bruder, A. M., & Taylor, N. F. (2023). Conservative interventions may have little effect on reducing diastasis of the rectus abdominis in postnatal women- A systematic review and meta-analysis. Physiotherapy, 119, 54–71. https://doi.org/10.1016/j.physio.2023.02.002
Do you work with people who have diastasis recti and want to learn more? Here are some resources for you:
Antony Lo @physicodetective: Diastasis Done Differently (self-paced online or in-person options available)
Grainne Donnally @absolute.physio: Diastasis Revolution: evidence-based evaluation and management (online)
Munira Hudani @munirahudanipt: The Diastasis Rectus Abdominis & Postpartum Core online course for professionals (online)
Did you like this blog? Here’s what’s next on your reading list:
Disclaimer: The information in this blog post is for general purposes only and is not intended to be used as medical advice, diagnosis, or treatment. Refer to your medical provider for all questions and concerns regarding your individual care.
Quick self-check
Curious if you might have pelvic floor dysfunction?
Take this quick self-screen. 10 yes/no questions, about a minute. Your answers stay on your device.

Did you enjoy this post? Whether you're a newbie or a pelvic pro, join the community to stay up to date with the latest and greatest in pelvic health!