Why So Many Patients Are “Hypermobile” - and what that means for their pelvic health
Why are so many pelvic PT patients hypermobile? A pelvic floor physical therapist explains the connection between hypermobility (hEDS/HSD), collagen, and pelvic floor dysfunction - plus a different, evidence-informed approach to treatment.

If you've spent any time in a pelvic PT clinic, you've probably noticed a pattern: a significant number of patients who come in for leaking, prolapse, pelvic pain, or painful sex are also hypermobile. Their joints move more than average. They may have been told their whole lives they were "double-jointed." They might have been the most flexible kid in gymnastics class - and they've spent years wondering why their body hurts so much.
This is not a coincidence. And as a pelvic floor physical therapist, understanding the connection between hypermobility and pelvic dysfunction is super important!
This is personal to me but my story is a bit unique. I have spent years with hypermobility and the ramifications, but it took me over 2 decades to figure this out. Why? Because I was not super-flexible with my muscles. I was never doing "circus-freak" party tricks. I could barely do the splits as a kid.
So, my muscle flexibility was "normal" but my joints were hypermobile. Which is why I had knee tendonitis for 5 years after riding my bike across Iowa and always hurt with long-distance running. My shoulders would sublux with walking (gravity!) and sleeping in sidelying. I've had surgery on both ankles to repair torn ligaments from too many sprains, a hip labral repair, knee surgery, etc. I have neck pain right now from "sneezing wrong" 2 weeks ago. 🙄 So while many of my hypermobile patients have had it way worse than me, I do empathize and I can relate!
What are we going to cover in this blog:
✅ What is "hypermobility"?
✅ Why hypermobility shows up so often in pelvic PT/OT
✅ How does hypermobility affect the pelvic floor
✅ Different treatment approaches to help people with hypermobility
✅ Reframing the narrative that "hypermobility" is akin to "fragility"
✅ Finding the right provider

So let's get into it: What Is Hypermobility, Really?
Hypermobility simply means that one or more joints can move beyond the normal range. When five or more joints are involved, it's called generalized joint hypermobility. It's important to note that hypermobility and joint instability are NOT the same thing - though hypermobile people are more prone to instability, subluxations, and dislocations.
Hypermobility is driven by a genetic difference in collagen, the structural protein that makes up our connective tissues:
ligaments
tendons
fascia
joint capsules
blood vessels
the gut lining
Think of collagen as the body's steel cable. In hypermobile bodies, that cable is a bit more like a bungee cord: it stretches easily, deforms under load, and takes longer to recoil. The result is a body that lacks adequate passive support - and has to work overtime to compensate.
When hypermobility causes symptoms, it becomes a "hypermobility syndrome" - most commonly:
Hypermobile Ehlers-Danlos Syndrome (hEDS)
Hypermobility Spectrum Disorder (HSD)
These two conditions are considered clinically equivalent. Research suggests they affect at least 1 in 500 people, though many experts believe the true prevalence is much higher, in part because the average time to diagnosis is 10-12 years (and 16 years for people assigned female at birth).
That diagnostic delay matters enormously. Many of these patients have spent years being told nothing is wrong, or that their symptoms are anxiety, attention-seeking, or just "the way things are." Restoring their trust in their own body's experience is often the first and most important part of treatment.
Why Hypermobility Shows Up So Often in Pelvic PT/OT
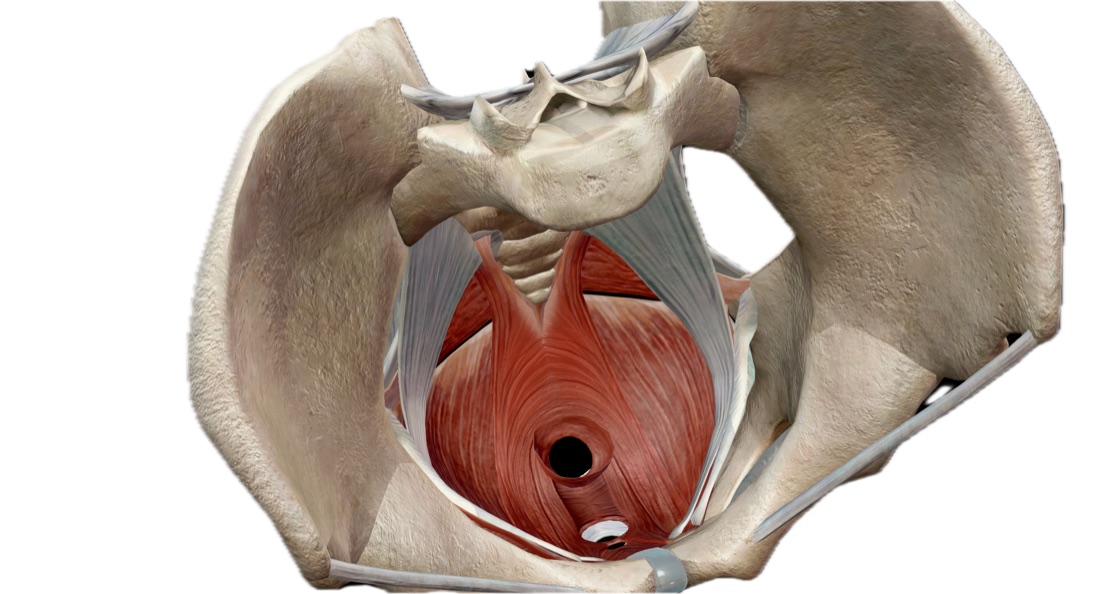
When connective tissue is lax throughout the body, the pelvic floor doesn't get a pass. The same collagen that supports your joints also forms the scaffolding for your pelvic organs, lines your blood vessels, and makes up the wall of your bladder and bowel.

Here's what that looks like clinically:
➡️ Urinary dysfunction: the most common complaint, affecting 60-73% of hypermobile people - compared to about 40% of the general population. This includes stress incontinence, urge incontinence, nocturia (waking to urinate at night), and urinary retention.
➡️ Pelvic organ prolapse: occurs at higher rates and at younger ages - sometimes in people in their 20s, with no history of childbirth. Without adequate collagen support, the walls of the vagina shift, and the bladder, uterus, or rectum can descend.
➡️ Pelvic pain: affects up to 50% of people with hypermobility syndromes - roughly six times the general population rate. Vulvodynia, painful intercourse, myofascial pelvic pain, and SI joint pain are all common presentations.
➡️ GI dysfunction: affects approximately 90.5% of people with hEDS in some form - constipation, diarrhea, IBS, bloating, and abdominal pain. This makes complete sense when you consider that the gut lining itself is made of connective tissue.
➡️ Perinatal complications: pelvic girdle pain in pregnancy, incompetent cervix, precipitous labor, hemorrhage, slower wound healing postpartum, diastasis recti, and a worsening of symptoms after delivery.
The Pelvic Floor Is Trying to Do Too Many Jobs at Once
Here's the key insight that changes how we treat these patients: the pelvic floor isn't weak - it's overworked.
When passive connective tissue support is inadequate, the muscular system compensates. The pelvic floor, along with the deep hip rotators, inner thigh muscles, and lower abdominals, picks up the slack - bracing, holding, and guarding in ways it was never designed to sustain. Over time, this chronic overload creates pain, trigger points, and dysfunction.
If we simply try to relax or release those tight muscles without addressing the underlying lack of support, we often make things worse. The muscles were doing a job. We have to replace that support before we take it away.
What Actually Helps: A Different Approach to Treatment
Treating hypermobile pelvic floor patients requires a thoughtful recalibration of everything we normally do. Here are the principles that guide my approach:
1. Evaluate in multiple positions:
A pelvic exam on a flat table doesn't always reveal what's happening in standing or during activity. Tissue creep - the gradual deformation of connective tissue under gravity - means symptoms often appear or worsen in upright positions. Assessment needs to reflect that.
2. Release AND rebuild - in the same session:
Manual therapy to address myofascial tension is often necessary, but it must be paired immediately with targeted strengthening. The goal is to give the pelvic floor new support - from the glutes, deep hip rotators, inner thighs, and lower abdominals - so it doesn't have to go right back to doing everything alone.
3. Start at a lower level, but progress higher than you expect:
Hypermobile patients fatigue faster, compensate earlier, and often don't respond the way typical patients do. A set of three reps done with perfect motor control is worth more than three sets of ten done sloppily. But here's the important counterpoint: research supports that higher-intensity loading is ultimately necessary to drive tissue adaptation. The goal is to get there - slowly, carefully, and sustainably.


4. Contain range of motion:
The bendy body loves momentum and end range. Teach smaller, slower movements in mid-range first. Slow down the eccentric (lowering) phase especially. Use tactile cues to help patients FEEL what the target muscle is actually doing. A metronome can be a surprisingly effective tool.
5. Add sensory input:
Because connective tissue laxity makes mechanoreceptors harder to stimulate, hypermobile bodies often need more sensory input to feel grounded and safe. This can come from taping, weighted vests, body braids, resistance bands, or self-massage - ways of providing that input WITHOUT stretching into end range, which only increases laxity over time.

6. Support is sometimes literal:
External tools like pelvic compression garments, supportive shorts, and pessaries can make a meaningful difference - not as a crutch, but as a way to offload the pelvic floor so it can actually train effectively. For patients with POTS (postural orthostatic tachycardia syndrome, which is very common in this population), abdominal and pelvic compression can reduce blood pooling and improve exercise tolerance significantly.
7. Recovery is non-negotiable:
Hypermobile patients have higher rates of delayed-onset muscle soreness and post-exertional malaise. Longer rest between sets, generous recovery between sessions, attention to sleep, hydration, and electrolytes - these are not luxuries. They are part of the treatment plan. Never progress at the expense of recovery.
8. Address the nervous system:
Anxiety, hypervigilance, and increased sympathetic arousal are common features of hypermobility syndromes - not just psychologically, but neurologically. The amygdala is often larger and more reactive. Chronic pain and instability keep the nervous system in a threat-detection loop. Breathing exercises, vagus nerve stimulation techniques, and education about pain neuroscience are all legitimate, evidence-informed parts of care.
Rewriting the Fragility Narrative
Perhaps the most important thing I can offer a hypermobile patient is a reframe. So many of them arrive having internalized the message that they are fragile, broken, or attention-seeking. They've tried exercise programs that left them flattened for days. They've been told to rest when rest made things worse, or to push through when pushing through caused flares.
When someone finally understands why their body responds differently - and that there's a specific, logical reason they don't respond to standard PT protocols - something shifts. They stop blaming themselves. They start being curious instead of afraid. That shift is the foundation of everything else.
Hypermobile people do get better. Not overnight, and not by following a generic protocol. But with the right approach, the right pacing, and a care team that actually understands their condition - progress is absolutely possible.

A Note on Finding the Right Provider
If you are hypermobile and dealing with pelvic symptoms, seek out a pelvic PT who has some familiarity with connective tissue disorders - or who is at least curious and willing to learn. When you call a clinic, it's completely appropriate to ask: do you work with hypermobile patients? Do you incorporate strengthening alongside manual therapy? Are you comfortable adapting exercise progressions for someone who fatigues quickly? In most states, you can access pelvic PT directly without a physician referral.
I hope this blog helped you gain insight about hypermobility disorders. Slow and steady strength training, avoiding long-distance and aggressive cardio like HIIT workouts, and other modifications have really helped me, but every hypermobile person is different and individualized care can make a huge difference!
You don't have to just live with this. There is help, and there is hope.
If you're unsure where to start or feel stuck with your progress, I'd love to help. I offer individualized assessments and strength-based treatments to help you return to the activities you love. 💛💛💛
If you live in the greater Minneapolis, MN area, schedule a consult with me or reach out if you have questions.
Resources:
Garreth Brittain, M., Flanagan, S., Foreman, L., & Teran-Wodzinski, P. (2024). Physical therapy interventions in generalized hypermobility spectrum disorder and hypermobile Ehlers-Danlos syndrome: a scoping review. Disability and Rehabilitation, 46(10), 1936–1953. https://doi.org/10.1080/09638288.2023.2216028
Engelbert RH, Juul-Kristensen B, Pacey V, de Wandele I, Smeenk S, Woinarosky N, Sabo S, Scheper MC, Russek L, Simmonds JV. The evidence-based rationale for physical therapy treatment of children, adolescents, and adults diagnosed with joint hypermobility syndrome/hypermobile Ehlers Danlos syndrome. Am J Med Genet C Semin Med Genet. 2017 Mar;175(1):158-167. doi: 10.1002/ajmg.c.31545. PMID: 28306230.
Yew KS, Kamps-Schmitt KA, Borge R. Hypermobile Ehlers-Danlos Syndrome and Hypermobility Spectrum Disorders. Am Fam Physician. 2021 Apr 15;103(8):481-492. PMID: 33856167.
Podcast - Zebra Talks: Living Your Best Bendy Life with Dr. Libby Hinsley, DPT @libbyhinsleypt
Did you like this blog? Here's what's next on your reading list:
How to Help Stress Incontinence: A Pelvic Floor PT's Guide to Understanding and Management
Exercise with Prolapse: what people and providers need to know
What to do for Diastasis Recti: A Pelvic Floor PT Perspective
Disclaimer: The information in this blog post is for general purposes only and is not intended to be used as medical advice, diagnosis, or treatment. Refer to your medical provider for all questions and concerns regarding your individual care.
Quick self-check
Curious if you might have pelvic floor dysfunction?
Take this quick self-screen. 10 yes/no questions, about a minute. Your answers stay on your device.
Did you enjoy this post? Whether you're a newbie or a pelvic pro, join the community to stay up to date with the latest and greatest in pelvic health!